What to do if you received a bill from a lab for services rendered at Family Care, PA.
If you are reading this, you probably received a bill from a lab and had a question, so you were directed to this blog post for answers. There are a few pieces of information you’ll want to collect before determining if the bill is accurate.
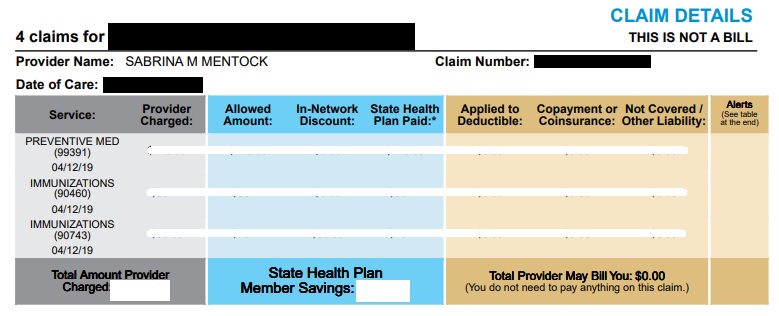
Check the Explanation of Benefits (EOB) letter from your Insurer. For any claim against your health insurance, you will receive a statement of benefits from your insurer after the claims has been processed. This is an insurance-side verification document to be sure you are being billed the proper amount from the rendering facilities. This document also explains why something wasn’t covered – in many cases, the reason is something that can easily be fixed once you review the explanation and compare the result to your plan’s details.
Seriously, check your EOB. This step answers 90% of the questions by itself and helps answer the other 10% much faster. Please take the time to find and evaluate a paper or electronic copy of this document before asking questions or paying a bill.
Check statement dates. If your EOB shows the claim was processed after the bill was generated, you may receive an updated bill to reflect the changes.
Check denial codes. If something wasn’t covered, the EOB will tell you why. If you disagree with the reason and think it should have been covered differently, you still have a chance to fix or appeal the denial. If the denial reason makes sense, you’ll likely owe that amount.
Check each line item. Often, large bills are the result of a single, uncovered service, among a set of otherwise covered services. Narrow your focus on the specific line items that need to be fixed in your appeal.
If your insurer does not have record of the claim (eg. there is no EOB), then the lab did not file your claim with your correct insurance. You will need to contact the lab to update your insurance information and have them re-file the claim.
Find the portion of the EOB that states your patient responsibility. Based on the denial reasons stated in your EOB, we may have the potential to appeal and/or re-file your claim to have it re-processed by your insurer. If you think there is something that should have been paid, this annotated portion of your EOB will give you a clue as to why the service was denied. From there, we have a few options. In order of most likely, here are a few of the common situations we encounter:
Amount applied to deductible.
This probably means the reason/diagnosis used for the testing was not considered a preventive code. If your bill shows a primary diagnosis code starting with a Z, it was probably filed as preventive. If not, many plans have a lab deductible to meet prior to covering non-preventive services. If you believe the service should have been considered preventive, read this information regarding preventive wellness services and/or check your insurer’s benefit package to verify potential coverage.
Coinsurance owed.
Even after you meet your deductible, many plans still have a coinsurance percentage that will apply to lab services. Instead of paying 100% prior to meeting your deductible, you will pay a smaller portion (usually 10% or 20%) until you reach your out-of-pocket maximum. Basically, if your insurer allows $10 for a service, you can expect to pay $1. If you have not yet met your out-of-pocket maximum, you should expect to owe some amount for all non-preventive services.
Non-covered services.
This service is not considered a part of your insurer’s benefits package. This is rare, but it does happen. In certain cases, mostly regarding lab procedures, the lab and/or your provider may not be allowed to bill you for non-covered services. Always contact the rendering provider of any non-covered service within 2-3 weeks of receiving your EOB to verify your claim’s status to be sure. For services that are ultimately considered non-covered and billable, we can potentially have you pay our uninsured prices, rather than paying the lab directly.
Still have questions?
If you have gone through these steps and still have questions, we would be glad to help! Please include a copy of your EOB, a copy of the bill you received from the lab, and any information you have learned so far from your discussions with your insurer and the lab. This information will be needed to solve whatever complication you’re having with your claim. Good luck!
The transcript below is a real email conversation I had with a patient who was trying to appeal a denied service. Reading this might help you avoid some of the delays we had with the appeal denial process and give you some direction on the steps you need to take if you want to file a claim appeal. The example refers to CPT Code 93880, which is a CIMT test performed at our office and often denied by out-of-state health insurance companies. You can potentially adapt the conversation to any CPT code, service, and price, as the process is very similar for appealing almost any denied service.
ME: We just received a denial for your CIMT test from February stating it was a “non-covered service” on your plan. That is the only information we received on our end – would you possibly be able to share the information on your statement with me so I can figure out if there is anything we can do for the appeal denial? Depending on why they determined it to be “non-covered,” we may have a few options available to get it covered. Thanks!
PATIENT: How much is it if it isn’t covered? I could dig into it a bit more, but if it’s hundreds of dollars, I’ll be extra motivated. 🙂 Are they usually covered by patients’ coverage?
ME: Yeah, it is usually covered. I was surprised to get the denial. It was $198.65, so it’ll probably be worth trying. I kind of enjoy trying to win these appeals, so I hope you’ll give it a shot! 🙂
PATIENT: I’d love to give it a shot! I’ll put that $200 to much better use. Is there any information I can send along in the meantime? I have had poor cholesterol and my family has a history of heart disease. The test revealed some unfortunate news about my “arterial age” and led to a cardiologist visit. Does that help my case? 🙂
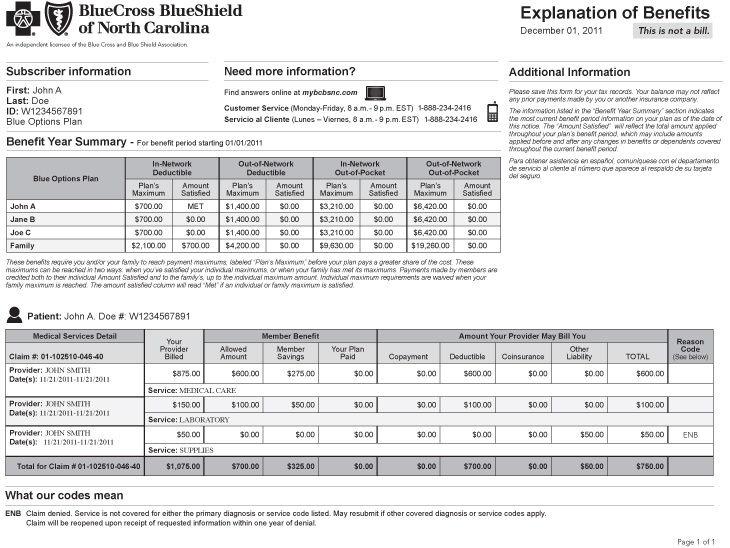
ME: Your EOB from your insurance will probably have more details – I have attached the version I received on my end. Can you see what details yours shows? I’m not sending you an invoice since I think we can get it covered, but I can if that might help. A letter of medical necessity is one of the last options we have for an appeal, so that information should help if we get to that point. Hope it is easier than that, but we’ll see what your EOB says and go from there. Thanks!
Eight Weeks Later (Act 2)
PATIENT: Still no EOB in the mail. I wonder if I’ll ever get anything. Could we move forward in some other way?
ME: Do you possibly have electronic-only EOBs enabled? Can you login to an account with your insurance and look at your claims?
PATIENT: Good thoughts. I do have access to my online account and there is an EOB in there! I attached it. There’s not much more in there, unfortunately. What can I do to help this effort?
ME: You may need to call them to get a better reason why it was considered non-covered. Sometimes, they just accidentally call it non-covered and as soon as you try to ask them why, it magically gets fixed immediately. The EOB is good to have if we’re filing an appeal, though, so that can be your proof of a denied claim (one of the three things they’ll probably need to initiate an appeal). I know it’s a hassle, but it’s really helpful to have an actual reason why it is non-covered before trying to submit anything just so we don’t run into the same problem after an appeal.
Someone at your insurer’s customer service department should be able to answer this question: “Why was CPT Code 93880 considered a non-covered service under my plan?” The process for an appeal denial is pretty much the same no matter what, but we’d give them different content depending on why they claim its non-covered. I hope that helps!
PATIENT: Great, thanks Ryan! I’ll give them a call soon and ask that exact question. I’ll be in touch.
Two Weeks Later (Act 3)
ME: Just an update to let you know BCBS requested all records related to the CIMT service. I just sent them about 20 pages worth of notes your provider thought were relevant, so we’ll see how they respond in about 4 weeks. You should get a long letter in the mail if it is denied again, or a short letter if they approve it. Your letter usually arrives about 2 weeks before ours, so let me know which you get and I can start fixing the new outcome a little sooner.
PATIENT: That’s great! Thank you for staying on top of this, Ryan. I have so much else to do during the day, I’ve been kicking the “call BCBS” can down the road. It sounds like they’re still in the process of determining whether it should be covered. I appreciate it, as always.
Three Months Later (Act 4)
ME: Have you heard anything yet? I received a appeal denial saying it was duplicate (meaning they didn’t change their mind about it being non-covered) a few weeks ago, but nothing else. Did you happen to get a full explanation of the appeal’s denial? Thanks!
PATIENT: Huh… you know, I never received anything more in the mail, and I never checked back up on my dashboard. I’m doing that now…Okay, done looking it up. It does look like I have 2 outstanding claims and I owe ~$200, but that seems lower than I recall it being. Both are for “Vascular Study.” Let me know if there’s any more info I can get you. I should probably pay this dang claim if I haven’t already.
ME: That kind of confirms what I got – just hoping for better news from you. I’ll send you an invoice so you can use your flex card to pay the balance. Thanks for the reply!
Last year, I wrote a comparison between the two options available to state employees through the NC State Health Plan to help people understand the differences between the plans and hopefully make a better decision when selecting a plan for their family. I’m updating that article for to include the changes for the 2019 NC State Health Plan here.
For the 2019 benefit period, North Carolina state employees have two possible choices for their health insurance plan: 70/30 and 80/20.
This article will cover the differences between the two plans and identify the types of families that would benefit from each option. I think the NC State Health Plan is one of the best health insurances you can have in North Carolina, so you are already somewhat ahead of the game with either option. However, because the two plans offer very different benefits, there is usually a “better” choice for everyone and the difference could be significant.
The plan did not actually change much for 2019, so I’ve essentially re-used most of my article from last year and updated it to include the new numbers. I hope this helps!
80/20 vs 70/30 NC State Health Plan Comparison
While most people focus on the cost of their monthly premium, that is not the only factor in your yearly healthcare expense. Sometimes, it makes more sense to pay a higher premium for better coverage if you know that you’re going to need that coverage during the year. Instead, you should try to minimize your total healthcare expense, which includes your premiums, deductibles, copayments, coinsurances, and other out-of-pocket expenses that you’ll have to pay during the year.
This is a direct, side-by-side comparison of the main financial factors that come in to play with these two NC State Health Plan options. While most people focus on the cost of their monthly premium, that is not the only factor in your yearly healthcare expenses. Sometimes, it makes more sense to pay a higher premium for better coverage if you know that you’re going to need that coverage during the year.
Instead of focusing on your premium payment, you should try to minimize your total healthcare expense, which includes your premiums, deductibles, copayments, coinsurances, and other out-of-pocket expenses that you’ll have to pay during the year. There are plenty of exceptions that apply to most situations, but understanding these key terms and aspects of the NC State Health Plan should help you make a reasonable prediction for your costs and set you up to figure out your own unique circumstances.
Below, I have split each of the factors into four basic sections:
Description of the term
The actual specs from each of the two plans
What the difference between the two plans means in concrete terms
And a “math” section that outlines how you can calculate your expected annual expenses using those numbers
Description: Your NC State Health Plan monthly premium is the simplest cost you’ll have to calculate. These are your fixed costs and the amounts you’ll be paying regardless of the real healthcare expenses you’ll have during the year. This number is 100% predictable, it does not change, and it is owed every month, no matter what.
70/30: $25/month ($300/year), or $598/month ($7,176/year)
80/20: $50/month ($600/year), or $720/month ($8,640/year)
Meaning: You can consider these numbers to be the “floor” of your annual health expenses. At the very least, if you have health insurance, you will have to pay your premium. If you never went to the doctor at all, you would have to pay at least $300/$7146 each year to be covered under the 70/30 plan.
Math: Multiply your premium by 12 months to get your annual expense.
Description: This is a flat rate, one-time expense that you incur with every visit to a medical provider for almost any reason. If you visit a PCP or specialist, expect to pay at least this much for your appointment.
70/30: $40 for Primary Care Provider; $100 for Urgent Care; $94 for a Specialist
80/20: $10 for Selected PCP or $25 for Any PCP; $70 for Urgent Care; $80 for a Specialist (a $35 increase from $45 in 2018)
Meaning: Try to predict how many times you’ll need to visit the doctor in a year and consider how much you will save from the difference in the copayment amounts. If you have been seeing the same doctor for a few years, they may be able to help you predict your expected number of visits and let you know what your provider’s plan for the next year might include.
Math: The 80/20 NC State Health Plan will save you $30 per visit to a PCP, $30 per visit to an Urgent Care, and $14 per visit to a specialist. Multiply your expected number of visits to each type of provider to figure out how much money you’ll save on your copayments by choosing to upgrade to the 80/20 plan.
Description: This is a variable rate that only applies after your deductible has been met. After you have met your deductible, you will owe this percentage of all health expenses incurred until you meet your annual out-of-pocket maximum.
A better way to think of the deductible/coinsurance relationship is to consider two periods: before you meet the deductible, and after you have met the deductible. Before, your coinsurance is effectively 100%, because you pay for everything. After, your coinsurance gets reduced to either 20% or 30%.
70/30: 30%
80/20: 20%
Meaning: If these plans were sold at a retail store, you might see this advertisement: “Buy $1,080 worth of healthcare and get your next $4,388 in purchases at 70% to 80% off!” After the plans reach their deductibles and coinsurance begins to apply, you’ll pay significantly less for every bill the rest of the year. Because you are paying more for the fixed cost of the higher premium, you’ll need to pass this point before the 80/20 plan eventually catches back up with the 70/30 plan for total expected expenses.
Math: Try to predict how many times you’ll need to visit the doctor in a year and consider how much you will save from the difference in the copayment amounts. If you have been seeing the same doctor for a few years, they may be able to help you predict your expected number of visits and let you know what your provider’s plan for the next year might include.
A decent estimate for visit costs would be $100 for a PCP visit, $200 for an Urgent Care visit, $300 for a Specialist visit, $500 for a MRI/CT, $2000 for an outpatient ER visit, and $5000 for an inpatient ER visit, per day. The 80/20 NC State Health Plan will save you 10% after your deductible, so you can add up the totals for however many of those services you’re expecting to use and discount 10% for the 80/20 plan to calculate your total savings.
Description: This is the amount in health expenses you’ll have to pay for before your insurance starts paying for the services you receive. Consider this a yearly down payment on your future care, to be paid as you go when necessary.
70/30: $1,080 Individual / $3,240 Family
80/20: $1,250 Individual / $3,750 Family
Meaning: Under either plan, you are on the hook for at least the first $1,080 in health expenses each year, with another $170 added under the 80/20. There are differences in copayments and prescriptions that mean the 80/20 plan will save you money in other ways during the year, but this will become a factor if you receive any of the wide variety of services that fall under your deductible.
Math: Once you know which services will be applied to your deductible, the cost calculation simply 100% of the cost until you’ve met your deductible. After your deductible has been met, your coinsurance will begin to apply.
I think the difference between the way out-of-pocket maximums are calculated carries one of the most important distinctions between the two plans, so I’m giving it a special section.
On the 80/20 plan, there is an “out-of-pocket maximum” of $4,890 for an individual (was $6,850 in 2018) and $14,670 (was $14,300 in 2018) for a family. This is the total amount of money, not including your premiums, that you would possibly ever have to pay for your healthcare in a single year. Even if you were in the hospital from January to December, this is the most you’d have to pay on the 80/20 plan (see assumptions).
However, on the 70/30 plan, there is no “out-of-pocket maximum.” Instead, the 70/30 plan has a cap on the “coinsurance maximum” at a $4,388 / $13,164 rate. Since we just covered how both plans have a deductible and the coinsurance applies to expenses after the deductible, you would think these would just be interchangeable terms. In a kind of sneaky way, this is slipped in as the biggest single category of expense for people who do end up meeting their maximums. Why?
Calling something an “out-of-pocket maximum” means it includes all deductibles and copayments. Literally, everything that the patient must pay for is included in that amount. When it is termed a “coinsurance maximum,” that very specifically applies only to patient responsibilities that are deemed coinsurance; deductibles and copayments are not included in this total.
Basically, you can interpret this to mean that the 80/20 plan only has a $3,640 “after deductible” coinsurance maximum that includes pharmacy benefits, while the 70/30 plan has a $1,080 medical deductible, $3,360 pharmacy deductible, and $4,388 coinsurance maximum separately. While the final out-of-pocket expenses are similar, the methods they each use to get there accumulate at different rates. Depending on where you fall on your expected usage, one side could still make a substantial difference.
Prescription Coverage
There are too many possible variables to really give a simple, universal estimate for prescription expenses, but I can at least guide you on how to figure out your own costs. It is easy to calculate the minimum ($0, because you don’t use prescriptions) or the maximum ($2,500/$3,360 when you reach your pharmacy maximum) expense, but everything in between is pretty much situational. To calculate your expected prescription costs per year, follow these steps:
Make a list of your medications. All of them, even over-the-counter meds and the ones you forget to take.
Look up every medication on your formulary. This is the document where you can find your drug’s “tier,” a hierarchical cost-based categorization system that the NC State Health Plan uses to decide how much you’ll pay for each drug. If you cannot find the drug, you will need to contact your insurer directly to ask about a more specific medication than they have listed in the general formulary. Estimate retail value for over-the-counter medications.
There are additional pharmacy resources linked at the bottom of this page.
Multiply the number of refills you’ll need by the copayments / out-of-pocket expense for each tier. You pay more for higher tier medications, so taking lower tiered or generic medications could potentially save a lot of money each year.
This is a somewhat oversimplified method, but it should give you a good starting point. There are a few other ways to reduce your costs:
If you take a Tier 2 or Tier 3 drug, contact your provider to see if a Tier 1 drug might be a suitable alternative. This may require an appointment or additional lab work, so take that extra cost into consideration.
If you expect to be taking the medication for at least the next three months, you may be able to get a cheaper, 90-day supply by using a mail order pharmacy.
If you don’t use GoodRx.com, sign up. We have discount cards at our office and would be glad to share – they send 1,000 of them every 3 months and we have way too many. Please, take them. I’ll give you 10, just in case you lose nine of them. Regardless of your insurance coverage, this site helps you find the best prices at different pharmacies and can save you hundreds of dollars on most non-formulary medications.
Necessary Details of the NC State Health Plan
This information should give you a good starting point for predicting your coverage, but it is not comprehensive. These are other categories of health expenses that you need to be aware of and factor in to your own personal calculations.
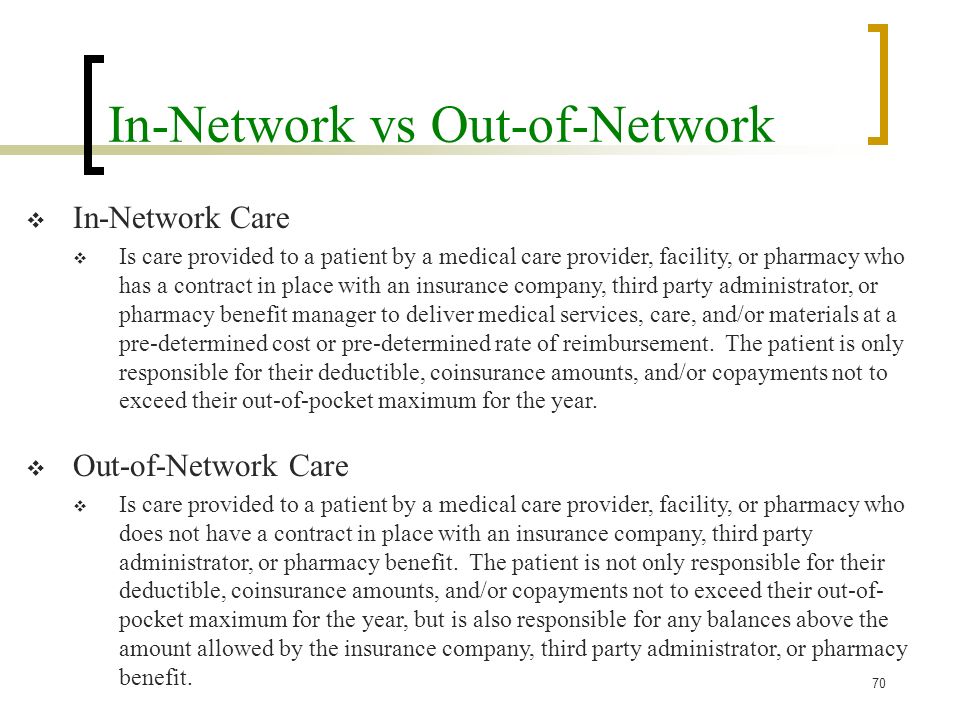
Out-of-network expenses. Visits to an out-of-network provider are “covered” under a separate set of benefits from your in-network out-of-pocket expenses. These benefits are usually at least 50% worse and there are a lot more things that are denied or non-covered, so it is best to stay in-network for almost anything you do.
The number of people covered in the Family plan. The “Subscriber + Family” option covers one kid, two kids, ten kids, or as many kids as you want to have. No matter how many kids are included, the Family Maximums are the same. If you consider the smallest “Family” to be 3 people, the price per person gets reduced significantly with every additional child.
3 people; $14,670 maximum = $4,890 / person, maximum
4 people; $14,670 maximum = $3,667 / person, maximum
5 people; $14,670 maximum = $2,934 / person, maximum
The amount of work you are willing to do. This especially applies to prescription coverage. Some of the most effective ways to save money will require you to call your insurer, fill out forms, document everything, track of receipts, and/or generally make you deal with your insurer’s customer service department. Assess how likely you are to make that effort, if needed.
Unexpected Expenses. You might get lucky, but remember that you are trying to predict 2019 health expenses for your entire family in October 2018. Things can change in the next hour, much less 2-14 months from now. If you choose the 70/30 plan, figure out how comfortable you are with having an accident and meeting the maximum, then consider that additional risk when selecting a plan.
Other NC State Health Plan Notes & Considerations
The “Free” Annual Wellness Visit is not included in the 70/30’s benefits, so your annual physical will have a $40 copayment just like any other visit. The 80/20 plan covers this at 100%.
For the 80/20 plan, Tier 3 drugs are applied to your normal deductible and coinsurance, instead of having a set copayment. While this probably makes the drug more expensive, having more expenses applied to a deductible is always a good thing for people who expect to hit their maximums. You could end up owing the pharmacy a lot of money early in the year, but then owe much less for all other health expenses combined for the rest of the year.
The 70/30 doesn’t cover ACA Preventive Medicines, either. Basically, you should just expect to pay more for birth control with the 70/30 plan, especially for branded medications.
Emergency room copayments are only a $37 difference, but the big part is in the 20% vs. 30% coinsurance owed. 10% of a single ER visit adds up quickly, so expect to pay at least $500-$1000 more for a single night’s ER stay with the 70/30 plan.
Your coinsurance kicks in sooner under the 70/30 plan ($170/$510 sooner for an individual/family plan), but your coinsurance rate is slightly worse. Because the 80/20 plan “catches up” with the 70/30 at a 10% rate, it would take $1,700/$5,100 in additional health expenses under each plan to reach a break-even point where you’ve paid the same amount in “deductible + coinsurance” under either plan.
The individual deductible on the 80/20 plan was reduced by $1,960, which is good news for everyone, but especially single employees with no dependents and families where one person generally uses most of the healthcare dollars on the plan.
Actions You Need To Take
It probably won’t be fun, but you still need to do this stuff.
Elect Your Plan. Kind of a weird way to say, “Choose a Plan,” but I guess we’ll go with calling it an election! You must choose the 80/20 or 70/30 plan. If you don’t make a choice, you will get defaulted to 70/30 and be charged an extra fee for the 70/30 plan for not making a choice.
Complete the Tobacco Attestation Credit. Even if you did it last year, you need to do it again. This saves you $60/month on your NC State Health Plan premium under every option.
Select a Primary Care Provider. There is a new link on the left side of your NC State Health Plan online account that allows you to change your PCP in just a few clicks. It was never too difficult to do over the phone, but any saved phone call to BCBS is a step in the right direction. We hope you choose Family Care!
Review Your Dependent Information. If applicable, make sure your spouse and kid(s) are enrolled on your plan. If you were married or had a kid since last enrollment, congratulations! Now make sure they are still on your plan! Double check that BCBS has demographic information like date of birth, mailing address, and phone numbers correct, as those can be a big hassle to correct later.
Print A Confirmation Statement. This is probably the most important thing you’ll do for yourself, so don’t skip this. I have heard so many nightmare stories and have listened to dozens of patients complain about being enrolled in the wrong plan on accident, and the only ones that I’ve seen win are the patients with their own receipts and records. Do not trust BCBS to get your information correct. Stay on top of it yourself and don’t let them make a mistake that costs you coverage, money, and sanity.
Summary
As with everything in healthcare, the standard “subject to individual determination” disclaimers always apply and nobody will, or should, give you a definite answer. I cannot tell you which plan you should choose, but I think you can use this guide to make that decision on your own.
All you can do is make the best estimate possible with the information you have at the time. Someone telling you they can accurately predict your actual health expenses is either lying, inexperienced, or delusional. Be ready to adjust if something does happen with your health and you need more extensive care than planned. Factor that potential into your decision and always be prepared for the worst-case scenario. I’ve found it is always better to be relieved things weren’t as bad as you thought, rather than being mad that they were worse.
For most people, your realized benefits under either plan will always be within a few hundred dollars of the other, so don’t stress out about the decision too much. This decision is not going to bankrupt you if you make the wrong choice. Either way, you will still have a plan that is better and cheaper than anything you could get on the individual marketplace.
Thank you for reading! I hope this helps you decide. Contact Ryan if you have any questions!
Good luck!
Assumptions
During the article, I left out mentioning many of the exceptions and individual circumstances that are possible with the NC State Health Plan. The article was already 3300 words, so I thought I’d save the trouble. Here are a few assumptions I made for all of the pricing and cost examples.
This is a breakdown of the distinct categories of expenses that you’ll have under either plan. Since it would be a little too confusing to talk about each of the 16 possible choices, I’m only using the “Subscriber Only” and “Subscriber + Family” plans as the low/high-end examples. You should adjust the numbers slightly if you choose the “Subscriber + Child(ren)” or “Subscriber + Spouse” options.
These numbers also assume that you will complete the Tobacco Attestation document and save $60/month on your premiums. If not, you should expect to pay an extra $720/year in premiums, but the rest of the expense calculations should remain the same.
I am also assuming you use a Blue Options Designated Specialist, visit your Selected Primary Care Provider for primary care services, and only visit in-network providers for all your healthcare needs. If you seek services under any other designations, you should expect to pay more.
Last year, I wrote a comparison between the three 2017 North Carolina State Health Plan options available to state employees to help people understand the differences between the plans and hopefully make a better decision when selecting a plan for their family. The State Health Plan (NCSHP) makes up our largest group of patients and I know it helped at least one person, so I figured it might be helpful to do the same thing this year. The information in last year’s article is still worth checking out if you are new to health insurance, in general, but this year should be a bit simpler.
Because the state eliminated the popular CDHP option for 2018 enrollment, NC state employees are left with only two possible choices: 70/30 and 80/20.
The rest of this article will cover the differences between the two plans and identify the types of families that would benefit from each option. I think the NC State Health Plan is one of the best health insurances you can have in North Carolina, so you are already somewhat ahead of the game with either option. However, because the two plans offer different benefit structures, there is usually a “better” choice for everyone.
80/20 vs 70/30 State Health Plan Comparison
This is a direct, side-by-side comparison of the main financial factors that come in to play with these two health insurance plans. While most people focus on the cost of their monthly premium, that is not the only factor in your yearly healthcare expenses. Sometimes, it makes more sense to pay a higher premium for better coverage if you know that you’re going to need that coverage during the year.
Instead of focusing on your premium payment, you should try to minimize your total healthcare expense, which includes your premiums, deductibles, copayments, coinsurances, and other out-of-pocket expenses that you’ll have to pay during the year. There are plenty of exceptions that apply to most situations, but understanding these key terms and aspects of your plan should help you make a reasonable prediction for your costs and set you up to figure out your own unique circumstances.
Below, I have split each of the factors into four basic sections:
Description of the term
The actual specs from each of the two plans
What the difference between the two plans means in concrete terms
And a “math” section that outlines how you can calculate your expected annual expenses using those numbers
Description: Your monthly premium is the simplest cost you’ll have to calculate. These are your fixed costs and the amounts you’ll be paying regardless of the real healthcare expenses you’ll have during the year. This number is 100% predictable, it does not change, and it is owed every month, no matter what.
70/30: $25/month ($300/year), or $598/month ($7,176/year)
80/20: $50/month ($600/year), or $720/month ($8,640/year)
Meaning: You can consider these numbers to be the “floor” of your annual health expenses. At the very least, if you have health insurance, you will have to pay your premium. If you never went to the doctor at all, you would have to pay at least $300/$7146 each year to be covered under the 70/30 plan. While the $720/month maximum premium seems steep, I would encourage you to try shopping for a plan on the individual marketplace and see exactly what kind of value you’re getting on the plan. The difference will probably be surprising. These premiums are very reasonable when compared with other options, especially considering the quality of the benefits of the plan.
Math: Multiply your premium by 12 months to get your annual expense.
Description: This is a flat rate, one-time expense that you incur with every visit to a medical provider for almost any reason. If you visit a PCP or specialist, expect to pay at least this much for your appointment.
70/30: $40 for primary doctor, $94 for a specialist
80/20: $10 for primary doctor (Need to visit Selected PCP); $45 for a Blue Options Designated specialist
Meaning: Try to predict how many times you’ll need to visit the doctor in a year and consider how much you will save from the difference in the copayment amounts. If you have been seeing the same doctor for a few years, they may be able to help you predict your expected number of visits and let you know what your provider’s plan for the next year might include.
Math: The 80/20 plan will save you $30 per visit to a PCP, $30 per visit to an Urgent Care, and $49 per visit to a specialist. Multiply your expected number of visits to each type of provider to figure out how much money you’ll save on your copayments by choosing to upgrade to the 80/20 plan.
Description: This is a variable rate that only applies after your deductible has been met. After you have met your deductible, you will owe this percentage of all health expenses incurred until you meet your annual out-of-pocket maximum.
A better way to think of the deductible/coinsurance relationship is to consider two periods: before you meet the deductible, and after you have met the deductible. Before, your coinsurance is effectively 100%, because you pay for everything. After, your coinsurance gets reduced to either 20% or 30%.
70/30: 30%
80/20: 20%
Meaning: If these plans were sold at a retail store, you might see this advertisement: “Buy $1,080 worth of healthcare and get your next $4,388 in purchases at 70% to 80% off!” After the plans reach their deductibles and coinsurance begins to apply, you’ll pay significantly less for every bill the rest of the year. Because you are paying more for the fixed cost of the higher premium, you’ll need to incur at least $1,700 in expenses AFTER you have reached your deductible before the 80/20 plan eventually catches back up with the 70/30 plan for total expected expenses.
Math: Try to predict how many times you’ll need to visit the doctor in a year and consider how much you will save from the difference in the copayment amounts. If you have been seeing the same doctor for a few years, they may be able to help you predict your expected number of visits and let you know what your provider’s plan for the next year might include.
A decent estimate for visit costs would be $100 for a PCP visit, $200 for an Urgent Care visit, $300 for a Specialist visit, $500 for a MRI/CT, $2000 for an outpatient ER visit, and $5000 for an inpatient ER visit, per day. The 80/20 plan will save you 10% after your deductible, so you can add up the totals for however many of those services you’re expecting to use and discount 10% for the 80/20 plan to calculate your total savings.
Description: This is the amount in health expenses you’ll have to pay for before your insurance starts paying for the services you receive. Consider this a yearly down payment on your future care, to be paid as you go when necessary.
70/30: $1,080 Individual / $3,240 Family
80/20: $1,250 Individual / $3,750 Family
Meaning: Under either plan, you are on the hook for at least the first $1,080 in health expenses each year, with another $170 added under the 80/20. There are differences in copayments and prescriptions that mean the 80/20 plan will save you money in other ways during the year, but this will become a factor if you receive any of the wide variety of services that fall under your deductible.
Math: Once you know which services will be applied to your deductible, the cost calculation simply 100% of the cost until you’ve met your deductible. After your deductible has been met, your coinsurance will begin to apply.
I think the difference between the way out-of-pocket maximums are calculated carries one of the most important distinctions between the two plans, so I’m giving it a special section.
On the 80/20 State Health Plan plan, there is an “out-of-pocket maximum” of $6,850 for an individual and $14,300 for a family. This is the total amount of money, not including your premiums, that you would possibly ever have to pay for your healthcare in a single year. Even if you were in the hospital from January to December, this is the most you’d have to pay on the 80/20 plan (see assumptions).
However, on the 70/30 State Health Plan, there is no “out-of-pocket maximum.” Instead, the 70/30 plan has a cap on the “coinsurance maximum” at a $4,388 / $13,164 rate. Since we just covered how both plans have a deductible and the coinsurance applies to expenses after the deductible, you would think these would just be interchangeable terms. In a kind of sneaky way, this is slipped in as the biggest single category of expense for people who do end up meeting their maximums. Why?
Calling something an “out-of-pocket maximum” means it includes all deductibles and copayments. Literally, everything that the patient must pay for is included in that amount. When it is termed a “coinsurance maximum,” that very specifically applies only to patient responsibilities that are deemed coinsurance; deductibles and copayments are not included in this total.
Basically, you can interpret this to mean that the 80/20 plan only has a $5,600 “after deductible” coinsurance maximum that includes pharmacy benefits, while the 70/30 plan has a $1,080 medical deductible, $3,360 pharmacy deductible, and $4,388 coinsurance maximum separately. While the final out-of-pocket expenses are similar, the methods they each use to get there accumulate at different rates. Depending on where you fall on your expected usage, one side could still make a substantial difference.
Prescription Coverage
There are too many possible variables to really give a simple, universal estimate for prescription expenses, but I can at least guide you on how to figure out your own costs. It is easy to calculate the minimum ($0, because you don’t use prescriptions) or the maximum ($2,500/$3,360 when you reach your pharmacy maximum) expense, but everything in between is pretty much situational. To calculate your expected prescription costs per year, follow these steps:
Make a list of your medications. All of them, even over-the-counter meds and the ones you forget to take.
Look up every medication on your formulary. This is the document where you can find your drug’s “tier,” a hierarchical cost-based categorization system that your insurer uses to decide how much you’ll pay for each drug. If you cannot find the drug, you will need to contact your insurer directly to ask about a more specific medication than they have listed in the general formulary. Estimate retail value for over-the-counter medications.
There are additional pharmacy resources linked at the bottom of this page.
Multiply the number of refills you’ll need by the copayments / out-of-pocket expense for each tier. You pay more for higher tier medications, so taking lower tiered or generic medications could potentially save a lot of money each year.
This is a somewhat oversimplified method, but it should give you a good starting point. There are a few other ways to reduce your costs:
If you take a Tier 2 or Tier 3 drug, contact your provider to see if a Tier 1 drug might be a suitable alternative. This may require an appointment or additional lab work, so take that extra cost into consideration.
If you expect to be taking the medication for at least the next three months, you may be able to get a cheaper, 90-day supply by using a mail order pharmacy.
If you don’t use GoodRx.com, sign up. We have discount cards at our office and would be glad to share – they send 1,000 of them every 3 months and we have way too many. Please, take them. I’ll give you 10, just in case you lose nine of them. Regardless of your insurance coverage, this site helps you find the best prices at different pharmacies and can save you hundreds of dollars on most non-formulary medications.
This information should give you a good starting point for predicting your coverage, but it is not comprehensive. These are other categories of health expenses that you need to be aware of and factor in to your own personal calculations when deciding on one of the State Health Plan options.
Out-of-network expenses. Visits to an out-of-network provider are “covered” under a separate set of State Health Plan benefits from your in-network out-of-pocket expenses. These benefits are usually at least 50% worse and there are a lot more things that are denied or non-covered, so it is best to stay in-network for almost anything you do.
The number of people covered in the Family plan. The “Subscriber + Family” option covers one kid, two kids, ten kids, or as many kids as you want to have. No matter how many kids are included, the Family Maximums are the same. If you consider the smallest “Family” to be 3 people, the price per person gets reduced significantly with every additional child.
3 people; $14,300 maximum = $4,766 / person, maximum
4 people; $14,300 maximum = $3,575 / person, maximum
5 people; $14,300 maximum = $2,860 / person, maximum
etc.
The amount of work you are willing to do. This especially applies to prescription coverage. Some of the most effective ways to save money will require you to call your insurer, fill out forms, document everything, track of receipts, and/or generally make you deal with your insurer’s customer service department. Assess how likely you are to make that effort, if needed.
Unexpected Expenses. You might get lucky, but remember that you are trying to predict 2018 health expenses for your entire family in October 2017. Things can change in the next hour, much less 2-14 months from now. If you choose the 70/30 plan, figure out how comfortable you are with having an accident and meeting the maximum, then consider that additional risk when selecting a plan.
Other State Health Plan Notes & Considerations
The state removed the “Free” Annual Wellness Visit from the State Health Plan 70/30 benefits, so your annual physical will have a $40 copayment just like any other visit. Last year, this visit to cover recommended preventive screenings and testing was covered 100% for all plans.
For the 80/20 plan, Tier 3 drugs are applied to your normal deductible and coinsurance, instead of having a set copayment. While this probably makes the drug more expensive, having more expenses applied to a deductible is always a good thing for people who expect to hit their maximums. You could end up owing the pharmacy a lot of money early in the year, but then owe much less for all other health expenses combined for the rest of the year.
The 70/30 doesn’t cover ACA Preventive Medicines, either. I am unsure how that law is being implemented or supported right now, but basically you should just expect to pay more for birth control with the 70/30 plan, especially for branded medications.
Emergency room copayments are only a $37 difference, but the big part is in the 20% vs. 30% coinsurance owed. A 10% difference in the bill from a single ER visit adds up quickly, so you should really expect to pay at least $500-$1000 more for a single night’s ER stay with the 70/30 plan in you have not yet met your deductible.
Your coinsurance kicks in sooner under the 70/30 plan ($170/$510 sooner for an individual/family plan), but your coinsurance rate is slightly worse. Because the 80/20 State Health Plan “catches up” with the 70/30 at a 10% rate, it would take $1,700/$5,100 in additional health expenses under each plan to reach a break-even point where you’ve paid the same amount in “deductible + coinsurance” under either plan.
If most of your health expenses come from prescriptions, the 80/20 plan will save you $860 between the $2,500 and $3,360 level. However, the advantage changes if you have more than one person in your family with high cost prescriptions. Under the 70/30 plan, the individual and family have the same $3,360 deductible, while the 80/20 plan has a $4,000 family maximum. If more than one person expects to spend ~$2,000 or more on prescriptions, the 70/30 plan will save you an extra $640 on those medications.
Actions You Need To Take
It probably won’t be fun, but you still need to do this stuff.
Elect Your Plan. Kind of a weird way to say, “Choose a Plan,” but I guess we’ll go with calling it an election! You must choose the 80/20 or 70/30 plan. If you don’t make a choice, you will get defaulted to 70/30 and be charged an extra fee for the 70/30 plan for not making a choice.
Complete the Tobacco Attestation Credit. Even if you did it last year, you need to do it again. This saves you $60/month on your State Health Plan premium under every option.
Select a Primary Care Provider. There is a new link on the left side of your NC State Health Plan online account that allows you to change your PCP in just a few clicks. It was never too difficult to do over the phone, but any saved phone call to BCBS is a step in the right direction. We hope you choose Family Care!
Review Your Dependent Information. If applicable, make sure your spouse and kid(s) are enrolled on your plan. If you were married or had a kid since last enrollment, congratulations! Now make sure they are still on your plan! Double check that BCBS has demographic information like date of birth, mailing address, and phone numbers correct, as those can be a big hassle to correct later.
Print A Confirmation Statement. This is probably the most important thing you’ll do for yourself, so don’t skip this. I have heard so many nightmare stories and have listened to dozens of patients complain about being enrolled in the wrong plan on accident, and the only ones that I’ve seen win are the patients with their own receipts and records. Do not trust BCBS to get your information correct. Stay on top of it yourself and don’t let them make a mistake that costs you coverage, money, and sanity.
Summary
As with everything in healthcare, the standard “subject to individual determination” disclaimers always apply and nobody will, or should, give you a definite answer. My wife is a state employee and I am making this same decision for my family, so you can consider this my way of talking out the decision for myself. I cannot tell you which plan you should choose, but I think you can use this guide to make that decision on your own.
All you can do is make the best estimate possible with the information you have at the time. Someone telling you they can precisely predict your actual health expenses is either lying, inexperienced, or delusional. Be ready to adjust if something does happen with your health and you need more extensive care than planned. Factor that potential into your decision and always be prepared for the worst-case scenario. I’ve found it is always better to be relieved things weren’t as bad as you thought, rather than being mad that they were worse.
For most people, your realized benefits under either plan will always be within a few hundred dollars of the other, so don’t stress out about the decision too much. This decision is not going to bankrupt you if you make the wrong choice. Either way, you will still have a plan that is better and cheaper than anything you could get on the individual marketplace.
Thank you for reading! I hope this helps you decide. Contact Ryan if you have any questions!
Good luck!
Assumptions
During the article, I left out mentioning many of the exceptions and individual circumstances that are possible with the NC State Health Plan. The article was already 3300 words, so I thought I’d save the trouble. Here are a few assumptions I made for all of the pricing and cost examples.
This is a breakdown of the distinct categories of expenses that you’ll have under either plan. Since it would be a little too confusing to talk about each of the 16 possible choices, I’m only using the “Subscriber Only” and “Subscriber + Family” plans as the low/high-end examples. You should adjust the numbers slightly if you choose the “Subscriber + Child(ren)” or “Subscriber + Spouse” options.
These numbers also assume that you will complete the Tobacco Attestation document and save $60/month on your premiums. If not, you should expect to pay an extra $720/year in premiums, but the rest of the expense calculations should remain the same.
I am also assuming you use a Blue Options Designated Specialist, visit your Selected Primary Care Provider for primary care services, and only visit in-network providers for all your healthcare needs. If you seek services under any other designations, you should expect to pay more.
How do I know if I am being billed the correct amount for my visit?
As most people can understand, figuring out exactly how much a particular medical service will cost can be extremely difficult. There are a lot of variables that factor in to the final cost of any care you receive, but it is still possible to get pretty solid information and set reasonable expectations for the most common types of services you will encounter. This post is designed to help you understand the basics of the billing process to help you identify any problems and know learn how to fix them.
When you are billed by any medical provider, they are usually working with the best possible information they can get about your insurance coverage at the time of service. However, regardless of how well they might be able to predict your coverage, providers are often still sometimes just as surprised as the patient when dealing with unexpected changes in coverage and quirks with different insurance plans. Because of this uncertainty, the amount you pay at the time of service may differ from the amount you actually owe.
No matter how much your provider may try to help navigate your insurance policy, the ultimate responsibility for the balance of a denied claim belongs to the patient. The total amount you will owe is called “patient responsibility” because you’re the one who will have to pay the bill and ultimately responsible for ensuring that you are paying the correct amount. Billing errors aren’t common, but they do happen and can be fixed pretty easily if you know how to find them.
PATIENT RESPONSIBILITY
There are three things that you’ll need to keep track of to know for sure if you are being billed the correct amount by your provider.
The amount you paid at the time of service.
The amount your explanation of benefits stated you would owe.
The amount of the bill you receive from your provider.
Ideally, #1 and #2 are equal and #3 never happens because you’ve already paid the correct amount for the service you’ve received after the appointment. For standard visits and simple insurance plans with copayments instead of deductibles, this is usually pretty easy. Your insurance says you’ll owe $25 for a visit, so you’ll pay your $25 when you check out and know that the rest will be covered. Easy. Unfortunately, there are far more instances where deductibles, co-insurances, exclusions, and other insurance hurdles will also apply to your benefits and make things more difficult to predict.
These types of “high deductible / shared percentage” plans are becoming much more common and make up all of the possible options available on the health exchange for Durham County in 2017. Because the total bills you’ll receive for these kind of plans are very much dependent on factors that you can’t guarantee before the service is rendered, the amounts you are charged for certain services are much more unpredictable.
This is where a basic checklist comes in handy:
#1. Remember what you paid.
Because most FSA plans now allow you to submit an electronic PDF of your receipts for tax purposes, you probably don’t need to save a real paper receipt of your transaction. However, you will still need to keep track of how much you’ve paid, just like any other bill you might have. You can also always refer back to your credit card statement or look at your online banking history to reference the charges, if needed. Either way, if you actually get a bill, you’ll want to look up previous payments towards your expected out-of-pocket expenses for that service and make sure they are already deducted from your total balance.
#2. Check your Explanation of Benefits (EOB).
This is a statement issued by your insurance company and either mailed or uploaded to your online member services account about 2-3 weeks after every claim filed on your behalf by a medical provider or facility. Your final out-of-pocket expenses are usually listed under a column titled “total patient responsibility” and will your insurer’s reasoning for each balance owed will be detailed on this document after your insurance benefits have been assigned to your claim. If you receive a bill because your insurer says your plan didn’t pay for something, this document will tell you why.
#3. Check your bill.
If you know what you’ve paid (shown on your receipt) and how much you should owe (based on your EOB), you can pretty much figure out how much you’ll be billed after the service.
Amount owed on EOB – Amount paid at time of service = Amount still owed
There are always exceptions at each facility you visit that may lead to separate fees associated with their services, but those are usually relatively minor compared to the total cost of care. If you think there is a problem with the amount you are being billed, be sure to contact your provider and double check to see if there are any other fees or balances that may have contributed to the difference before attempting to contact your insurance.
FIXING A PROBLEM
So, you’ve looked at your EOB and examined at your bill and the two numbers still don’t match up. Or, worse, they do matchup and the amount is significantly higher than you were expecting. Now that you have identified a potential discrepancy with the bill, what do you do about it? Your first phone call depends on where you find the problem.
My EOB and the bill from my provider both show the same amount due.
This is a problem between you and your insurer. In this case, the problem would be that you disagree with the amount your insurer said you would owe since your provider’s information matches the insurer. This means that the problem lies at the start of the claim process where your insurance assigned your plan’s benefits to the claim they received. You thought you would owe one thing, but your insurance said something else.
Here are the steps you should take to work towards a solution:
On your EOB, look up the “Remark Code” for the line items that are being denied. These are generally 2 or 3 digit alphanumeric codes that reference a longer explanation of denial later on in the document. This is a summary of the actual reason your insurance is using to deny this charge. If this summary explanation does not make sense to you based on how you understand your policy, you can call your insurance company for a full explanation.
When you call customer service, be sure to have your insurance card and EOB in front of you so you can reference the date of service, amount billed, and the specific line item that you are questioning. They will be able to look up your insurance policy and re-examine the specific claim you are referencing at the same time to make sure your plan’s benefits were applied correctly.
If your benefits were applied correctly, the representative can answer questions about your plan and help you understand how your benefits will be applied in the future so you can possibly avoid the same situation next time. Sometimes, payment is denied because they need to update information about your insurance plan, so you can answer their questions over the phone and take care of the balance in just a couple minutes. Learning more about your policy and how your insurance will process a similar claim could make a big difference in the long run.
If your benefits were not applied correctly, the customer service representative should be able to notice the mistake and submit your claim for reprocessing. If this happens to be the case, you’ll want to get a reference number for the call and notify the provider that sent you a bill. The insurance will likely give you a quote like “we will reprocess this claim and send a corrected claim to your provider in 2-3 weeks.” Whenever they give you a timeframe, double it and then call your provider back to see if everything has been resolved.
My EOB says one amount owed, but the provider’s bill says something different.
If you have carefully looked at your receipt, EOB, and billing statement and still think there is a problem that is unrelated to how your insurance processed the claim, here are several logical explanations, in order of potential likelihood:
You owed money for another claim. Most of the time, your billing statement only includes claim details for the claims with a balance owed. It is possible that your provider applied part of a payment you’d made to a claim that is not currently on your billing statement because that balance was covered.
You paid $100 at the time of service, but $40 went towards a balance from January and $60 went towards a balance from April. Because you also owed $100 from the April visit, you may receive a bill for $40 for that claim even though you paid $100 already.
You owed money for additional fees and services not on the bill. Every practice is different, but there are always additional fees that you may have to pay for services that are not reimbursable by insurance companies. These include charges for things like missed appointments, form completion, records requests, and certain lab tests that aren’t covered by insurances. Part of a payment you made may have been applied to one of these types of charges.
You had a previous credit applied. Sometimes, the system actually works in your favor and you might overpay for a charge up front. When this happens, you’ll receive a credit on your account that may be applied to future balances and reduce the amount you are charged at the time of service. If you were unaware of the credit, you may have expected a service to be cheaper than you thought when you paid.
You overpaid by $20 a couple months ago, so your provider only charged you $5 for your usual $25 copayment. When you look at your EOB, it shows that you would owe $25 for that visit, even if you only paid $5 that day.
There was a mistake. Most financial correspondence between your insurer and provider is electronic and automated, but that doesn’t mean there aren’t mistakes. As the provider, we receive batches of claim data that includes dozens of claim rows and about 20 columns of payment information per claim from the insurer and we have to sift through every row, column, and number to ensure its accuracy. As you can imagine, it is very tough to get through this process and end up 100% perfect. Even at 99.9% accuracy, that means an average primary care facility will generate about 10 incorrect patient balances per month. Before getting upset or worried about the possibility of owing for a service, have your provider double check the claim first before attempting to appeal through your insurer.
You can easily identify which one of these situations is likely to apply to you by asking for a “transactional summary” of all your claims for a certain time period. All providers may call this report something different, so you’ll just need to ask for something that shows all the charges on all claims filed by the provider and how all of your payments were applied to your account over a certain time period. This will let you see, line by line, what caused the problem.
Most of the time, any changes to a bill with an amount that differs from your EOB will always be initiated by the provider who performed the service, so it’s best to start at the source if you want to fix a potential problem. I hope this has given you the knowledge to better understand your medical bills and the confidence to discuss them with your provider, if needed.
If you have any questions related to the content of this article or if you’ve experienced any other type of situation that I didn’t address, I’d love to read your comments below. Thanks for reading!
To help all of the State employees of North Carolina figure out which version of the State Health Plan would be best for them during the upcoming year, I thought we would attempt to review the differences between the three options – CDHP (85/15), Enhanced 80/20, and Traditional 70/30. The State has developed a very informative site with lots of details and specifics for the State Health Plan, so I won’t repeat anything you can find there. The goal of this post is to compare, line by line, what the numbers associated with each plan mean and which types of medical situations end up being the preferred option financially for each person once all expenses have been considered.
All State Employees should have received a “Decision Guide for Open Enrollment” packet from their insurer for the 2017 benefit period sometime in the past few weeks. You can use the “2017 State Health Plan Comparison” table on Page 8 in this booklet, or you can click on this link to get the PDF online. Here we go!
2017 North Carolina State Health Plan Comparison
HRA Starting Balance: You’ll notice that the CDHP plan is the only option with an Health Reimbursement Account (HRA). An HRA is basically a fund that your employer sets aside to pay for your qualifying medical expenses. With the CDHP plan, an individual has their first $600 in health expenses paid through their employer’s HRA. This is basically free money, as long as you need it and use it for things that are approved by your plan (eg. doctor’s visits, most prescriptions). Effectively, this splits the CDHP’s $1,500 deductible into two different periods, where you end up only having to pay once you hit $601 in expenses each year.
One thing to consider is that you actually need to use $600 in health expenses for this aspect of the plan to help. If you don’t use it, the $600 set aside for you in your employer’s account usually resets and lets the employer keep any unused funds to help reduce expenses the following year. While $600 is the same to anyone, this is an especially nice feature for people who expect their total health expenses to be less than $600 per year because they’ll never have to pay anything except their premiums.
Annual Deductible: A deductible is the amount of money you will have to pay out-of-pocket for non-preventive services before the actual benefits on your insurance plan will start to take effect. Of the three options available, the 70/30 has the lowest deductible, but that doesn’t mean it is the best plan. This means that the plan’s benefits kick in earlier, but the 70/30 plan also has greater expenses after the deductible and a much higher out-of-pocket maximum than the other plans. Other than just the dollar amount, there are two distinct differences in how these deductibles are applied:
The CDHP plan applies all medical expenses to the deductible. Your sick visits, specialist appointments, prescriptions – everything goes towards your initial $1,500 deductible. Other than the covered ACA Preventive Services, this plan doesn’t pay any of your health care expenses until after you have met the deductible.
The 80/20 and 70/30 plan have co-payments for PCP visits, urgent cares, and prescriptions so the deductible only applies to things like surgeries, labs, and hospital visits. While the deductibles are lower, they are also less likely to be met because they only apply to certain things.
Co-Insurance: You might notice that the co-insurance rate is also indicative of the name of the plan – eg. the 80/20 plan features a 20% co-insurance. The co-insurance is a percentage that requires the patient to pay a certain portion of approved medical services once their deductibles have been met. Basically, as a reward for paying 100% of everything out-of-pocket before you met the deductible, your insurance will now start helping pay your health expenses by reducing your portion to either 15%, 20%, or 30%, depending on the plan. Once you have met your deductible, this is the percentage of your health expenses you will be required to pay until you have met your co-insurance maximum.
Medical Co-Insurance Maximum: The 70/30 plan is the only one that has a medical co-insurance maximum. The other plans have their own maximums, so while this seems like a small bit of semantics, but it actually makes a pretty big difference in your possible expenses. The CDHP only has a combined out-of-pocket maximum that includes co-insurance and pharmacy benefits, while the 80/20 plan skips the co-insurance maximum and separates the out-of-pocket maximums between medical and pharmacy. By calling it a “co-insurance maximum” and not a “out-of-pocket maximum,” this number does not include the annual deductible that has already been paid.
This graphic does not include the separate prescription deductibles associated with the 80/20 and 70/30 plans.
Because the $4,350 out-of-pocket maximum in the 80/20 plan includes the $1,250 deductible, the 80/20 plan’s effective “co-insurance maximum” is really only $3,100. With the 70/30 plan, you’ll be paying the $1,080 deductible PLUS $4,388 more. A small difference, but one that costs over $1,200 if it actually comes into play. Also, it is important to remember that the 80/20 and 70/30 plans have separate deductibles for prescriptions, which we will get into soon.
Medical Out-of Pocket Maximum: As mentioned in the previous paragraph, the medical out-of-pocket maximum includes all out-of-pocket expenses a person would have to pay for medical services each year. This includes co-payments, co-insurances, and deductibles. For the 80/20 plan, this means you’ll have a cap on your medical expenses each year of $4,350. Because this number includes the deductible, you’ll basically be paying a $1,250 deductible, and then +20% of the next $15,500 in health expenses you incur (for a total of $4,350). This number puts a cap on your total annual medical expenses, so you can consider this the limit of a “worst case” scenario (not including prescription coverage).
Pharmacy Out-of Pocket Maximum: This is just like the medical out-of-pocket maximum described above, but only for prescriptions. The 80/20 plan and 70/30 plan both have separate deductibles for prescriptions, while the CDHP plan assigns both medical and pharmacy claims towards the same deductible. This makes it seem like the CDHP plan has better prescription coverage than the 80/20 or 70/30 plan, but those two only apply their deductibles to high tiered prescriptions that aren’t used by very many people. With the 80/20 and 70/30 plans, most of your prescriptions will be a set price for a 30- or 90-day supply, so most people will never really get close to meeting their limits with simple $5 and $30 co-payments per month.
Out-of-Pocket Maximum (Combined Medical and Pharmacy): The basic concept was covered in the previous two sections, but this number represents the “worst case scenario” for all of your out-of-pocket health expenses combined. There is no scenario where an individual will have to pay more than $3,500 on the CDHP plan, $6,850 on the 80/20 plan, or $8,828 on the 70/30 plan. This is a helpful number to know if you’re going to need a major surgery or hospitalization. These numbers are relatively low compared to today’s health insurance environment, where standard maximums are usually around $10,000 or $15,000 annually, so this is a one of the best aspects of the State Health Plan and a major selling point for most people.
ACA Preventive Services: These are the rates for certain services that have been categorized as “preventive” by stipulations in the Affordable Care Act, which has been adopted by the State Health Plan. You can check out the details of what is considered a preventive service on the State’s website – this includes things like your annual wellness exam, most vaccinations, and standard age-based guidelines and screenings. Preventive medicine has been proven to keep people healthier, so insurer’s are making a big push to ensure all of their members get these basic, cost-effective primary care services now so they can avoid having to pay for complicated, expensive hospital visits later. Because the services are preventive, and not urgent, the insurance penalizes you significantly for receiving these services out-of-network, so make sure the provider you see accepts your insurance if you want to receive these benefits.
Office Visits: So far, everything has basically seemed most favorable to the CDHP 85/15 plan. The next few topics are where the real benefits of the 80/20 and 70/30 plans come in, since they have co-payments for most medical services, instead of a deductible. While their deductible may be higher, it also applies to fewer things that you are likely to need. This is also the part of your benefits that applies to appointments at Family Care, if you were wondering.
For example, consider a single primary care visit for the flu – to make it easy, we’ll say its your first visit of the year.
With the CDHP plan, you are paying 100% of the cost of the visit because you haven’t met your deductible yet. This includes the doctor’s visit, flu testing, lab work, prescriptions, and any other services you may need. However, if the visit falls within the first $600 of your annual health expenses, the charges would be paid by your HRA account and you would not owe anything out-of-pocket. You would also get $25 added to your HRA, so you can think of that like a cash-back rebate towards your health expenses for using an in-network provider. After your HRA has been exhausted for the year, you will owe 100% of every office visit you have for the next $900, and 15% after that until you reach your maximum.
With the 80/20 plan, you would only pay a $25 co-payment for a doctor’s office visit, rather than having the charges applied to your deductible and owing 100%. Basically, you would save about $75 every time you went to a PCP and $215 every time you went to a specialist. If you had any testing or additional services (eg. flu test, breathing treatment, etc.), your deductible would apply in addition to your co-payment. This makes things relatively simple and helps people budget costs once they expect to have several office visits each year.
The 70/30 plan has the highest co-payments, but they are still not too far off from the 80/20 plan and the deductible applies to PCP visits the same way. You will have a higher co-payment, but still pay the same rates for additional services towards your deductible.
Urgent Care: Just like the section on Office Visits, but in an Urgent Care setting. There isn’t too much different about the basic process from office visits, so the main thing to notice is how much higher your expenses will be at an urgent care vs. your primary care provider. Whenever possible, you should always try to visit your primary care provider before attempting to go to an urgent care. For example, at this great independent primary care facility known as Family Care, we can guarantee either same-day or next-day appointments, so we can help you avoid the higher costs and lower quality of service that you’re bound to experience at an urgent care facility.
The nice thing is that the benefits for urgent care visits are identical at both in-network and out-of-network providers. Because the problem you are experiencing is obviously “urgent” if you are visiting an urgent care, your insurance company won’t care about the network and allow you to get treated wherever is most convenient. They charge a steep fee for this convenience, but it is still nice to know you won’t be charged more because of the network.
Emergency Room: Again, the CDHP plan applies charges to a deductible, while the 80/20 and 70/30 plan have co-payments associated with the visits. Depending on the significance of your reason for visiting the ER and how close you are to meeting your deductible, either one might be considered the best option for your situation. The one, and probably only, benefit to an ER visit is that you’ll likely go well beyond your entire out-of-pocket in just a few hours, so your healthcare will basically be “free” for the rest of the year. Yay for you!
Inpatient Hospital: This is reserved for actual hospital stays where the patient is admitted and kept in the hospital for some period of time. With all of the plans, you’ll only end up receiving the benefits in this row if you visit the ER and are then later admitted to the hospital. The insurance does not try to charge you twice after an admission, so the bump from an ER visit to an admission is not too drastic. The CDHP and 80/20 plans have an option to either get money back or have their co-payments waived if you visit a Blue Options Designated Hospital, so you should try to visit a preferred hospital whenever possible.
Prescription Coverage: The concept of tiers is pretty complicated, so I will go over this part in a separate post. However, the basics are still pretty much as the regular medical benefits the same across the three options. The CDHP has prescriptions applied to the same deductible as everything else, while the 80/20 and 70/30 plans have co-payments associated with different tiers of drugs. If you aren’t sure what these terms really mean, here is a good 2.5 minute video on what a drug formulary is and why your insurance has grouped different drugs into tiers.
For the State Health Plan, specifically, here are the links to the specific formulary for each plan. You should look up the medications you take to determine what tier they are classified under so you can get a good idea of your expected costs for that drug. The formulary changes all the time and the difference between a Tier 1 drug and a Tier 2 drug could be hundreds of dollars per year, so this helps keep you from being surprised when you show up at the pharmacy.
In my opinion, the State Health Plan is the best health insurance to have in North Carolina. Each plan has their specific benefits and drawbacks, but they are all significantly better insurance plans than the plans you’re likely to find available on Healthcare.gov. The problem is finding the plan that makes the most sense for how it will actually be used by you and your family. Every medical situation is unique, but here are some of the pros and cons of each plan to might help you make your final decision.
CDHP (85/15)
Pros: Potential for $0 premium and includes the lowest cost to add children and/or spouse. If you spend under $600 per person, your out-of-pocket expenses will be paid entirely by your HRA. This plan has the lowest out-of-pocket maximum, so this plan has the best “worst case scenario.”
Cons: You are required to pay for 100% of your expenses between $600 and $1,500 each year. You’ll have to pay for prescriptions under the same deductible as medical expenses. You’ll need to take additional steps to set up your HRA with your employer.
Enhanced 80/20
Pros: Lowest co-payments for PCP and Urgent Care visits, as well as most prescriptions. Pharmacy deductible is only $2,500, so meeting that deductible could help reduce overall costs if prescriptions make up a large percentage of your medical expenses.
Cons: Requires at least $15 per month, minimum, in premiums and has the highest premium cost to add family members. Potentially has the highest cost in a situation where multiple family members need extensive care and prescription coverage.
Traditional 70/30
Pros: Has a lower premium than the 80/20, but still maintains a similar structure for PCP and urgent care visits. Has co-payments for Tier 3 medications, so certain medications might be cheaper than the other plans. One prescription deductible applies to the entire family.
Cons: Has the worst coverage after the deductible has been met of the three plans. Because the premium is similar to the CDHP, while the coverage is similar to the 80/20 plan, the segment of people that would have the best coverage for their unique situations is fairly narrow. Most people would be better off getting the CDHP or 80/20, but there is a definite middle group where this plan makes the most sense.
I hope this was a helpful breakdown of the major components of these three plans. For more details on how you should think about this information, in general, be sure to check out our recent post on the 3 things you should consider when signing up for health insurance.
If you have any questions, please submit them in the comments and I’ll be sure to reply. Thanks for reading!
3 Things to Consider When Signing Up For Health Insurance
The problem that most people have with their health insurance plan is rarely with the actual coverage – people are generally only upset when their plan doesn’t cover something they thought it would or when they are surprised by some costly detail that wasn’t made clear at enrollment. Insurance companies don’t do the best job of educating patients on the actual details of the plans they are selling, but the information you need to know to set proper expectations is available if you know where to look. You’ll have to do some work and learn some pretty boring things, but you are the one who ultimately has to understand the details of your plan’s coverage, not your insurer. The point of this article is to help you understand the crucial differences between possible plans and help you feel comfortable with the coverage you choose.
The entire concept of health insurance is that you are basically making a bet on your health. The healthier you are, the less likely you are to use your insurance for high cost medical services. Your insurance company knows this and sets their prices accordingly. If the insurance company thinks you are going to cost $5,000 to cover this year, their goal is to set your total premiums and out-of-pocket expenses to more than $5,000 so they can make a profit.
This is the bet –who will get the better deal once all of your medical expenses have been paid?
The benefit structure of every plan offered by insurers is carefully calculated to give them the best chance of winning this bet. By understanding how your insurance plan works, you can put the odds back in your favor and make every dollar you have to spend on healthcare go much further.
There are three broad categories to consider when signing up for a new health insurance plan:
Cost – How much will I pay in out-of-pocket expenses?
Coverage – What services and medications will I have access to under my plan?
Network – Is my provider “in-network” with my insurance plan?
Each component is equally important and can have critical implications on the others. While it is almost impossible to get your expected costs 100% right before things actually happen, just having a very good estimate will help you budget accordingly and avoid surprises when you seek medical care. If you need help with this calculation, our Health Insurance Cost Estimator Tool should help give you a good estimate.
I hope the following pages will help you fully understand the benefits, and consequences, of your choices when you’re deciding between two possible plans.
Continue reading to go into further detail on each one of these components.
COST – How much will I pay in out-of-pocket expenses?
The most popular way to think about the cost of your health insurance plan is to focus on the monthly premium. This sounds good because you know the fixed costs associated with your plan and can seemingly predict exactly how much you will have to spend for coverage. However, this line of thinking leaves out the most important part by ignoring the variable costs a person might incur each year when they actually use their health insurance and visit their doctor.
To get a complete picture, you should compare a plan’s total expected out-of-pocket expenses, which factor in the possible copayments, coinsurances, and deductibles that you might have to pay for during the year in addition to your premiums. Signing up for insurance and paying your premiums to your insurer is not the only out-of-pocket expense you should expect if you need medical care. Much like car loan payments don’t cover the cost of the gas you need to put in the car, different health insurance plans might require significantly more “gas” than others if you actually want to take your plan out for a drive.
There are two primary things to consider when comparing the cost of two different plans – how much you’ll actually use your insurance, and how much you’ll have to pay in a “worst case scenario.” It is also important to remember that the out-of-pocket maximum does not include premium payments. Here is a quick plan comparison as an example.
Plan A:Higher Premium, Lower Out-of-PocketIf you have some chronic conditions that require frequent visits to specialists and take some high priced medicines, it will probably end up being cheaper to pay a higher premium for better coverage. Since you’ll be using the insurance often, it is comforting to know you’ll have a low limit on out-of-pocket costs when you actually need care. However, if you don’t end up using your insurance as much as you thought, you’ll be paying significantly more for unnecessary coverage.
Plan B:Lower Premium, Higher Out-of-PocketIf you are relatively healthy and rarely visit the doctor, a cheap premium with a high deductible makes sense because you want the lowest fixed costs possible. By not seeking medical care often, you can be pretty sure your variable costs will be low. You leave yourself more vulnerable to higher costs if something bad were to happen, like an unexpected emergency room visit or hospital admission, but that is a part of the bet you’re placing on your care.
Now to the fun part – Charts! Woo!
This chart compares the total cost of the healthcare you need with the total out-of-pocket expenses incurred if you were covered under either Plan A and Plan B. Because Plan A has a higher premium, the fixed cost of this plan has a higher floor than Plan B. If you don’t actually need to use the insurance, you will save money by choosing Plan B. The turning point occurs when the two lines intersect, which in this comparison is just over $4,000 in total health expenses. At that point, you’ll be saving money by choosing Plan A, even though the premiums will be more expensive.
Remember that “bet” we talked about earlier between you and your insurance company for who has to pay more of your healthcare expenses? The grey line represents the actual expense incurred to keep you healthy. As you can tell, the insurer is hoping they have enough members incur less than about $7,500 in health expenses each year to pay for the few members who will be extremely expensive to cover. The insurance wants to move that break-even point as far to the right of the chart as possible, while you’re hoping to intersect with their line as close to the left as possible.
Because it is impossible to predict the future and know exactly what services you’ll need, the best way to look at something like this is in terms of a “Best Case” / “Worst Case” scenario.
In a “Best Case” Scenario, where this person is perfectly healthy and never uses their insurance plan at all, Plan A will be twice as expensive as Plan B ($4,800 vs. $2,400) because the premiums are guaranteed payments regardless of how often you use your insurance plan. Plan A will actually still be more expensive than Plan B, overall, all the way up to the first $4,000 in out-of-pocket expenses. If you are unlikely to have at least $4,000 or more in annual health expenses, it makes sense to pay a lower premium and pay more of your own out-of-pocket expenses. Plan B would be a better choice as long as your expenses were lower than $4,000 during the year.
In a “Worst Case” Scenario, where this person ends up in the hospital for at least a few days and racks up $50,000+ in medical expenses, Plan B will be up to $2,600 more expensive because there is a higher deductible and out-of-pocket maximum limitation. The ACA put a cap on the out-of-pocket maximum that a patient would have to pay in such a situation, so the out-of-pocket maximum helps provide a safety net to ensure people don’t go bankrupt due to a medical emergency. In this case, Plan A would have better coverage.
These are overly simplified examples, but it shows how the total cost of healthcare for an individual can vary greatly just based on the type of plan they choose. Most likely, you will fall somewhere in the middle of the “Best Case” / “Worst Case” spectrum. The goal is to guess how close you are to one side or the other and how likely it is that you’ll need a high cost service during the year. You obviously can’t plan on having a serious accident, but the closer you get to that tipping point between the two plans, the more you might want to consider increasing your coverage to feel a little more comfortable with your financial risk in such a situation.
COVERAGE – What services and medications will I have access to under my plan?
There are several different ways to define “Coverage” when you’re referring to the details of an insurance plan, but this section will focus on the specific procedures, treatments, and prescriptions that your health insurance plan will approve. Basically, if you have a problem and you sign up for an insurance plan, you want to make sure that specific problem is something that falls under the benefits outlined in your plan.
The majority of what is required to be covered by insurances is either mandated by the Affordable Cart Act or derived from basic Medicare standards, so most of coverage details for medical services are the same across the major commercial insurers. But, that doesn’t mean they are all the same, either. Standard medical services like doctor’s visits, generic medications, and vaccines, will be accepted on almost any plan. However, if you are planning to do non-standard things, like cosmetic surgeries, treatment for rare or complex diagnoses, or special blood testing, you should really try to dig a little deeper into the plan to see what types of services are actually covered.
Essentially, the best way to think about how to get the “best” coverage you need is to start by seeking coverage for your most expensive service. Call your providers and ask for a price quote for certain types of visits you expect to incur during the benefit year. You will probably never get a definite answer (for a variety of really good reasons that we’ll answer in another post), but you should be able to get a ballpark idea what kind of prices you can expect. Ask for the specific CPT Codes that will be used for your procedures so you can tell your insurer exactly what you want to verify. Then, figure out which insurance plan covers the services that would cost the most if you didn’t have coverage because they will make the biggest difference in your bottom line for out-of-pocket expenses.
Here is a simplified chart that helps you visualize the types of priorities you should be making when selecting coverage. These are just working estimates and are by no means exact, especially considering that we just spent 1,000 words earlier in this article talking about how the “Cost If Covered” part of the equation could vary drastically depending on your plan. The point is to get a sense of the risk involved in having, or not having, coverage for a particular service.
Obviously, having coverage for the ER visits would be Priority #1 in this scenario. A single accident with no coverage could be financially devastating. But, those are generally few and far between for most people. Again, this goes back to the concept of placing a bet on your health expenses. You should go down the list of your expected health costs and find a plan that will pay for all of your highest priced items first, since they will have the biggest net difference on your potential bottom line.
After all, what would be worse? Having to pay an extra $75 because a PCP visit was denied, or having to pay an extra $45,000 because your hospital visit was denied? A PCP visit is more likely to occur, but the one time the hospital visit gets denied will potentially be the most devastating. However, because denials are still not too common if you have insurance, the most common factor that comes up when differentiating plans based on their overall coverage relates to prescriptions, as they can vary greatly depending on the plan.
Prescription Coverage Details
One plan could offer a certain drug at a $10 copay, while another plan might not cover it at all and either cost you $200 out-of-pocket or force you to switch to a different medication that your insurance prefers. Neither option is ideal, as you’re ultimately either poorer or sicker if your medication isn’t covered by your insurance. The insurers structure their drug coverage decisions based on the population of their insured, so finding the plan that best suits your patient profile could make a big difference in prescription costs.
So, how do you find out which drugs are covered on which plan?
To be confident in your choice, you should learn the details of the prospective plan’s drug formulary. Most of the time, a simple Google search with “Name of Insurance Plan, Drug Formulary List” in the search box will direct you to a PDF of the plan’s details. If not, there should a link on the insurance provider’s website or a phone number you can call to request a copy by mail or email. Prescriptions are one of the few health expenses you can make an accurate budget for up front, so it is important to know how your plan will cover the medications you are currently taking.
If you think your medication may be too expensive, even with commercial insurance, there may be programs that you can sign up for to reduce the cost. Please contact our office to discuss potential coupons, savings programs, and rebates that may be available for your medication. There are a lot of programs available to receive discounted prices on your medications, so it is ultimately in your best interest to take advantage of them when you can. If you are a current patient, ask for details!
NETWORK – Is my provider “in-network” with my insurance plan?
If you already have certain medical providers you prefer and want to make sure you’ll still have access to those providers, you’ll want to sign up for a plan that is accepted as an in-network insurance by your provider. If you stay in their provider network, the benefits on your plan will actually apply to your visits and you’ll receive a much lower rate than you would if you went out-of-network.
Because a person may see multiple providers and every provider has their own list of accepted insurances, you may run into a problem finding a single plan that is accepted by all of your preferred providers. Or, once you find that plan, you realize it is just way too expensive and cannot afford to sign up, so it is effectively inaccessible. In this situation, you’re going to need to make some type of compromise. You should start by assessing the true cost of the care you expect to receive and focusing on your largest possible expenses first.
No matter where the line of “affordability” lies, it is obvious that a PCP visit is at least “more affordable” than an emergency room visit. If you had to pay for one of those yourself, you’d much rather it be the $100 PCP visit rather than the $5,000 ER visit. While you can still manage to incur some pretty significant medical costs with frequent primary care offices and specialists, the out-of-pocket expenses will never be on the same level as a single visit to the hospital. Because primary care visits at Family Care average around $100 per visit if they are not covered, you’d have to have non-covered primary care visits twice a week for an entire year to match the cost of a single accident that landed you in the hospital.
With most health expenses, the bills escalate quickly due to a few common types of services:
Hospital Visits. Just one night in the hospital could cost more than $10,000 if you don’t have insurance, so these visits create the majority of medical debt.
Surgeries. A single surgery can sometimes cost more than $5,000 and often requires several costly follow up visits to make sure you are recovering well.
Tiered Medications. For drugs that have very specific indications or are considered upper-tier level medications, out-of-pocket costs can be up to $1,000 per month.
Because we are dealing with a situation where the insurance company is putting the obligation to pay the claim on the patient, this is basically an extension of our previous discussion on covered services, in general. Being “out-of-network” is one of the most commonly used reasons for an insurer to deny coverage for a particular service, so your plan’s network really has a big influence on your expected out-of-pocket expenses for a certain service. For example, the price of the same EKG at an out-of-network cardiologist could be 500% more expensive than if it were performed by an in-network cardiologist. That is actually kind of crazy when you think about it, but that is for another article.
There are a few different ways to find out which providers are in your network.
Call your insurance company. There is always a customer service number you can call to speak with a representative from your insurance. Ask them to send you a list of the providers in your area that accept your insurance. Usually, they will either read you a list over the phone, email you PDF file, or direct you to the content on their website.
Visit your insurer’s website. Most insurance plans have a “Provider Finder” tool somewhere on their website. Make sure you select the proper choices from all of the possible search filters to ensure that the list actually applies to your plan.
Call the provider. Each provider will know which plans they accept, so you could ask them as a starting point. Make sure know the name of the company (eg. BCBS, Cigna) and the name of the specific plan (eg. Blue Advantage, Choice Plus), as both of those are required to verify your coverage. Even if the provider says they accept your plan, you may want to double check with the insurer, anyway, as they will be the ones to ultimately process your claim and make that decision.
In order to maximize the amount of coverage you receive from your plan, you should try to stay “in-network” for as many services as possible. Plan to be “in-network” for the big expenses first, because that will make the most difference in your yearly out-of-pocket spending. There are many plans that actually offer pretty good out-of-network benefits, but they will still always be at least some margin less than your in-network benefits.
TLDR – A summary of the most important pieces of this article.
To summarize the last 3000 words, here are the main points I hope you learned from this article:
Your monthly premium is not the only factor you should consider when signing up for an insurance plan. You should consider your total out-of-pocket expenses, which include any copayments, coinsurances, and deductibles associated with the plan you choose.
The amount of money you have to pay each year can vary dramatically from one plan to another. You should try to estimate your expected health expenses for the year and find a plan that works for you.
You should seek coverage for your highest priced services first, and then worry about the lower priced items later. It is much easier to pay a $100 PCP visit out-of-pocket than it is to pay a $5,000 hospital bill.
If you are on medication for a chronic condition, you should ask to see a prescription drug formulary for your prospective plan to ensure that the medication you need will be covered by the plan you choose.
You should try to visit in-network providers whenever possible. Going out-of-network can significantly reduce the amount of benefits you will receive from your insurance plan.
If you are a current patient at Family Care and have any questions, you should ask Ryan for help! Contact us here.
VIDEOS – You prefer to watch videos about health insurance instead of reading articles? OK!
Because I completely understand that most people consider insurance to be completely boring and tedious, I tried to select some fun insurance education videos that I thought were actually pretty entertaining. These videos cover similar concepts to what we just discussed in this post and help emphasize the most important point of this whole article – that health insurance can be a good thing that actually make sense and occasionally helps you out, if you know what you’re doing. I hope you learn something that helps you even the playing field and get the most out of your coverage.
HUMANA – “How Do Deductibles and Copays Work?”
This is a really cool whiteboard “explainer” video on the different possible ways you could incur out-of-pocket expenses. I think this video does a good job on the concept of out-of-pocket maximums and deductibles, while making you really care for Gina as a person. At 1:59 in the video, I blame whoever was supposed to be spotting Gina on the ladder for that accident. It is also pretty cruel to just leave Gina on the ground while telling her she owes 20% of her medical bill for the fall. C’mon, video guy.
KAISER FAMILY FOUNDATION – “Health Insurance Explained – The YouToons Have It Covered”
This video covers the interesting journey of a beanie-wearing skateboarder that signs up for health insurance and gets into an accident because of a thieving raccoon. The video does a really good job explaining the risk factors involved with not having insurance and understanding the value of staying in-network for services. In the end, you’re actually a little bit upset the hero of the story didn’t learn from his experience when he chases after the raccoon again. You’re gonna get hurt again, dude! Let the raccoon go!
“MILIMAN, INC – Understanding healthcare costs: The employer-sponsored insurance system”
For the roughly 2/3 of people who don’t really care about the individual healthcare marketplace because they have health insurance through their employer, this video is for you. This helps explain the reason your premiums rise, or why your employer changes your plan every year to put more of the cost burden on the employee’s out-of-pocket expenses. Most of the time, if your individual contribution is increasing, your employer’s contribution is also increasing. It might not always be at the same rate, but just something to think about so you don’t always have to blame your company for being evil. The video also has a little bit of a “Tron” feel to it, so that is also kind of cool.
“GOATS ON A STEEL RIBBON” – Goats On a Steel Ribbon.”
You’ve probably had enough about insurance for one day, so you deserve a treat. These are goats on a steel ribbon. It is hilarious and mesmerizing and I really wanted the big goat to jump on the ribbon. I like to imagine that big goat jumped up on the ribbon just after the camera stopped recording and he is still there today, happier than all the goats in the land. You can do it, big goat!
Family Care, PA is a primary care medical facility located in the Durham, North Carolina. We understand that there are a lot of options for primary care in the area, so we know we need to provide a great service if we want to earn your trust. The large local hospitals are still very good, but we think that we provide a special type of care and attention to every patient that is not possible inside such a large system. Here are a few of the reasons we think you would really enjoy having Family Care as your primary care provider.
We get to know you personally. Our medical staff and providers take the time to get to know you during your visit, rather than rushing you through your appointment. You will never feel rushed during your visit and will have the opportunity to fully explain your symptoms and concerns. Our administrative staff also takes the time to get to know our patients and works with them to overcome common healthcare hurdles like coordinating specialist referrals, obtaining prior authorizations, requesting medical records, and appealing claim denials.
We are great patient advocates. At Family Care, being the best advocates possible for our patients is always our priority. When coordinating care, we always try to work within the structure of your insurance coverage to make sure the process is smooth and you are able to receive the full extent of your plan’s benefits. Our office policies regarding scheduling appointments, payments, and paperwork are all designed to provide the most efficient and affordable care possible.
We utilize available technology. Our office is able to provide efficient care by taking advantage of the wealth of technology available in healthcare today. We use an Electronic Medical Records system to manage our practice, which features an online patient portal. The portal provides 24-hour per day access to their own medical records at our office, including appointment reminders, prescription directions, and historical lab results.
We schedule 30 minute appointments. Unlike most primary care offices, we schedule each of our visits in 30 minute blocks of time. This does not always mean your visit will actually take a full 30 minutes, but the extra allowance does help make sure you are seen on time for your appointments and still have plenty of room to explain the full nature of your visit and concerns to your provider.
We are up front about our policies. We try to make the processes for how we provide efficient medical care as open and transparent as possible so our patients can understand the reasons behind them and why they are necessary, and beneficial, for our patients. We do our best to help patients understand their insurance policies and are always open about expectations, likely possibilities, and potential problems with obtaining coverage in certain situations.
We are able to be contacted easily. If there is anything else you need to know, just call our office at 919-544-6461. Family Care does not use a “phone tree” or automated operating system, so a real employee at our real office will pick up the phone when you have a question. If we aren’t able to answer the call, it is simply because we are at lunch (12pm – 1pm), or are helping another one of our patients in the office. If you leave a message, we will call you back shortly. Or, you can also contact us by…
Signing up for our patient portal and submitting a message directly to your provider through our EMR system.
Flying a drone to GPS coordinates “Latitude: 35.915967, Longitude: -78.894075″ with your hand-written message. Please print.
Note: Mention this option at your next visit and Ryan will give you a piece of candy.
We are grateful for the opportunity to take part in your medical care. We understand that you have plenty of options available to you – Durham is the “City of Medicine,” after all. We try to help in every way possible and hope you truly enjoy visiting our office. Thank you for giving us a chance to provide you with great medical care!
Insurance Terminology 101: “Approvals” and “Authorizations”
One commonly misunderstood concept about insurance coverage is the term “approval.” It seems pretty simple, but many people think that having a service approved by their insurance plan means that they will not have to pay for the service. While that is possible depending on the situation, the most often result is that the patient is left surprised and confused when they ultimately receive a bill for an “approved” service. This post is part of a series to help patients clarify the terminology that your insurance company is using so they can better understand their coverage.
Approval / Authorizations
Approval by an insurance plan means that they will allow you to get something done and will at least consider paying for the test. This does not mean that your health insurance will pay for the test – it means they agree that the procedure will be subjected to the benefits listed on your insurance plan. Authorizations are essentially the same thing as approvals, but you’ll hear authorizations more often with prescription coverage details. Just like approvals, a prescription authorization only means your insurance benefits will be applied to the claim for your prescription and does not guarantee payment.
While you may still be paying for an approved service, your insurance company at least acknowledges that this test or medication is generally recommended for your particular medical situation and should be considered as part of your plan’s benefits. They are not saying they won’t pay yet, but they also aren’t saying they will pay, either. This is the first chance in the claims process for your insurance company to get out of paying for a service, so getting this approval is a good first step.
However, obtaining an approval does not mean you will not still owe up to 100% of the service you are approved to receive. Your benefits for an approved service could include deductibles, coinsurances, copayments, and additional out-of-pocket expenses that you will have to pay the service’s provider. If you have a high deductible that has not been met, for example, you will still incur a large out-of-pocket expense for approved services.
—–
Let me know what you think in the comments section below. If there are any other phrases or terms that you sometimes get confused, please send me a message and I’ll try to feature your question on a feature post. Thanks for reading!
One of the most common problems that people experience with their health insurance is the frustration of having to pay out-of-pocket for a service or prescription that they thought would be covered by their insurance plan. “I thought that was covered” is a common phrase with patients and most of the negative perceptions of health insurers stem from the general distrust that this reaction causes. People are skeptical about insurers covering certain things because they have been burned in the past and see insurers as being greedy whenever they end up owing more than just their premiums for their healthcare expenses. While insurers do sometimes make mistakes and deny things that should be rightly covered (which you have the right to appeal), your insurance is usually processing your plan’s benefits exactly how they said they would when you signed up for the plan. They probably even have your signature on a sheet of paper saying you agreed to their terms. Sneaky, I know.
The problem usually begins because patients misunderstand their coverage and get surprised when they see the differences in benefits from what they thought they would have to what they actually have. The new Farmers Insurance commercials are really a perfect example. Knowing your coverage could influence your decision on where and when to get treatment and help you reduce your overall out-of-pocket expenses. It will also keep you from being surprised with unexpected bills or regretting services that you wouldn’t have done if you knew the cost. You may even change plans entirely because you realize your coverage is terrible, or if you are paying too much to have coverage for services you don’t need.
Because all plans are unique, it is impossible to make a single guide that covers everyone to determining your coverage. This post is designed to help you understand the thought processes and terminology behind determining your plan’s details so you can navigate through your own insurer’s information with a good idea of what you should be looking for.
Which health insurance plan do you have?
This is probably one of the first questions you’ll have to answer and is the starting point for all other questions you’ll be asked in every possible healthcare situation. When someone asks you what health insurance you have, what do you say?
Example Insurance Card
There are two things your healthcare provider or pharmacist is always looking for when they ask this question.
The name of your insurance provider. This is the most basic starting point and 100% necessary for your provider to determine your plan details. Examples include Blue Cross Blue Shield (BCBS), CIGNA, Aetna, United Healthcare, etc.
The plan type and/or name of plan. This is the first subsection of the insurance provider and describes the plan option you chose when signing up with your insurer. Sometimes the plan has an actual name. Examples of BCBS plans include Blue Advantage, Blue Value, Blue Options, Blue Saver, State Employees Health Plan, etc. The plan could also only be described by letters, like PPO, HMO, POS, EPO, etc.
Depending on the situation, your provider might also need some additional information. Typically, you will be asked for the rest of this information if you are going to be receiving medical services or prescriptions, if you need a prior authorization for anything, or if you are being referred to another doctor.
Your Subscriber Number. This is the first basic identifier on your insurance card. It may also be called your Member Number, Identification Number, or something else similar. This is the biggest and most important number on your card, so it is probably highlighted in some way. If you have dependents on your plan, the Subscriber Number includes the two digit suffixes assigned to each dependent. For example, Dad could be ABCD0000-01, Mom could be ABCD0000-02, and Daughter could be ABCD0000-03.
Your Group Number. This is usually the second most featured number on your insurance card and allows your provider to see which pool of subscribers has a similar plan. This is usually unnecessary for most purposes, but is generally required if you need a prior authorization so it is good to have on file. The group number also helps providers figure out your plan details when you have private employer-based plans or some of the more obscure plans available that they might not see that often.
The Payer ID # or the Billing Address. This is necessary for billing your insurance, but most providers already know the proper way to bill your insurance provider and don’t necessarily need it if you have a popular insurance plan. If your plan is based out-of-state or if you have a smaller, more obscure plan, you will probably be asked for this information. The Payer ID # is a 5 digit number on the back of your card and should be somewhere near the Billing Address.
That information will help your provider process your claims, send referrals, and obtain necessary prior authorizations. It will not allow your provider to tell you how much you will owe for a service or what types of benefits you have on your plan. Knowing your basic plan details only guides your provider so they can use the proper channels to correctly process your insurance benefits – it will not help them predict what those benefits will be, or even if there are benefits allowed for a service, at all.
Because plan details can vary on an individual basis, it is impossible for your provider to predict your benefits with complete certainty. We process the claims at the time of service with every piece of verifiable information we have available, but there are always surprises.
For example, you may pay a $20 copay for your visit. Then, after your plan processes the claim and says you are not covered for that service, you find out that you are required to pay 100%, instead. This is why it is important for you to know your own coverage – you are the person that is impacted by how your claims are processed and are ultimately responsible for any surprises that happen with your plan, so it is best to avoid them!
What are my benefits for this service?
The primary thing everyone wants to know – how much do I have to pay for this? There are several methods you can use to figure out your plan’s details for a particular service and the types of benefits you can expect to receive.
Look at your insurance card. This is a “snapshot” of your coverage and usually shows the most pertinent details of your plan. The problem with relying on this is the lack of detail and explanation for your coverage for specific services, or the types of exclusions or exceptions that may be active on the plan. With most plans, this shows what you’ll need for the majority of the services you’ll receive.
Reference your enrollment paperwork and benefits package. Whenever you sign up for a new insurance plan, your insurance provider is obligated to send you a detailed package that includes your plan’s coverage benefits. This is usually sent within a couple weeks of your enrollment and may be updated each year with a new packet of information. Usually, there is a table of information included with three columns – the service type, the plan’s in-network benefits for that service, and the plan’s out-of-network benefits for that service. Whenever you visit a provider or facility, reference their section on this table to help predict what your benefits will be for that visit.
Contact your insurance provider. On the back of your insurance card, there should be a customer service number that you can use to ask any questions you may have about your plan. They will always give you a standard “this call does not guarantee payment of services and benefits will be subject to the plan’s details at the time of service” spiel to make sure they aren’t promising coverage they can’t provide, but they should be able to tell you what your copayments or deductibles are and how they apply to certain types of providers and services. Most plans have online portals with customer service emails or live chats, as well, but the process is the same. You’ll want to contact your provider for the CPT Code they will use for the service and ask your provider specifically about your benefits for that code.
Look at how previous visits processed under the same plan. Past coverage is a good predictor of future coverage, but only if the plan’s details have not been changed. If you had a $25 copayment for a sinus infection six months ago, and your plan has not changed since then, you will probably owe a $25 copayment for a sinus infection today. This could be a little problematic because it refers to your benefits at a previous date, rather than your benefits today, so make sure your plan details have not been modified since the service you are using as a reference.
Just hope something is covered and deal with it later. This is probably the worst option, but it is usually the one most people end up choosing because they are either intimidated or frustrated or confused with the process for actually understanding their benefits. Because this experience just ends up perpetuating the “patient-versus-insurance” mindset, when the two should be working together towards the mutually beneficial goal of reducing the cost of healthcare, I hope this post helps people avoid this option!
This was a basic summary of ways you can determine the details on your insurance plan. This is the fourth post in a series on understanding the insurance claim process. In the rest of the blog posts in this series, I will explain the specifics involved in your EOB, including detailed information on the following topics:
If you have any specific questions or topics you would like us to discuss, please mention them in the comments below and we will address them in future posts. If you are a patient at Family Care and have any questions about EOBs you received for claims from our office, please let us know by filling out our contact form. Thank you!
This is the third in a series of posts about the insurance claim filing process. The process can be daunting and seem confusing, but the basic components are fairly easy to understand if you break them down individually. The goal is to help our patients, and everyone else, understand what is actually happening “behind the scenes” when you use your health insurance. You can read the rest of the series by clicking on the link headers at the bottom of the post.